How the cochlear implant (bionic ear) functions
 Clark’s first research aimed to see if electrical pulses could reproduce the time code for sound frequencies. His experimental work showed the brain stem nerve responses could follow electrical stimuli from 1 pulse per second and 300 pulses per second. Note that at high rates, the nerve responses disappear, indicating that a single channel implant would not be satisfactory for a cochlear implant.
Clark’s first research aimed to see if electrical pulses could reproduce the time code for sound frequencies. His experimental work showed the brain stem nerve responses could follow electrical stimuli from 1 pulse per second and 300 pulses per second. Note that at high rates, the nerve responses disappear, indicating that a single channel implant would not be satisfactory for a cochlear implant.
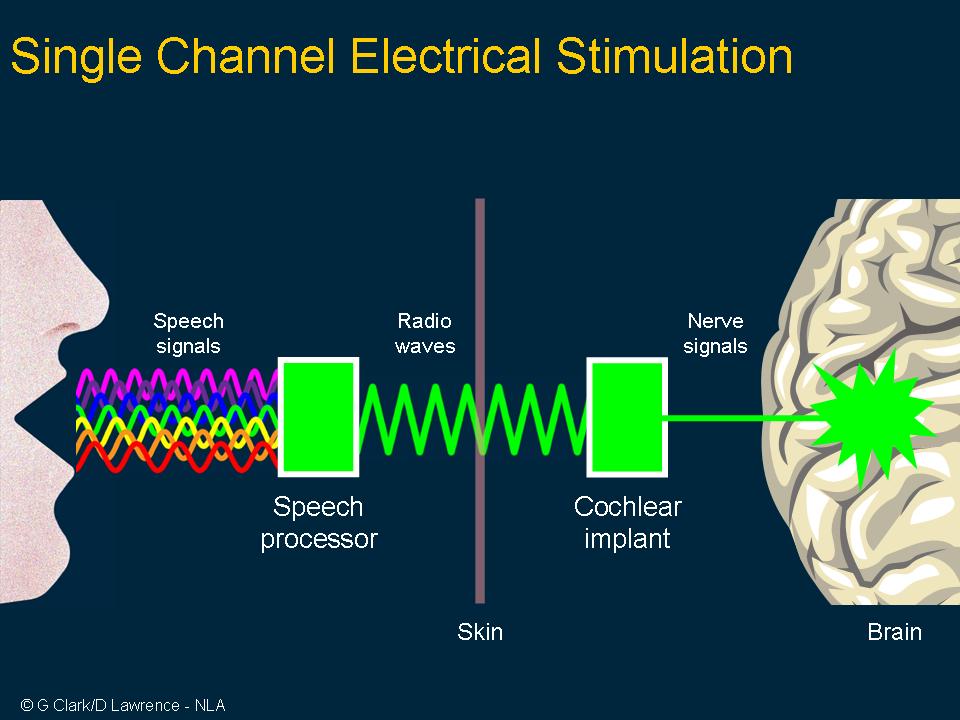 A single channel implant as shown here would only convey the amplitude envelop of speech but not the frequencies needed for speech comprehension.
A single channel implant as shown here would only convey the amplitude envelop of speech but not the frequencies needed for speech comprehension.
 There was thus an electro-neural bottleneck for getting frequency information through to the brain by temporal coding. For that reason, he developed research for place coding so that selected speech features could be transferred through the bottleneck.
There was thus an electro-neural bottleneck for getting frequency information through to the brain by temporal coding. For that reason, he developed research for place coding so that selected speech features could be transferred through the bottleneck.
 In order to produce the range of pitch (frequencies) and loudness (intensity) needed for speech understanding, multi-channel stimulation, or cochlear implant, was required. This was the significant innovation established by the University of Melbourne research team.
In order to produce the range of pitch (frequencies) and loudness (intensity) needed for speech understanding, multi-channel stimulation, or cochlear implant, was required. This was the significant innovation established by the University of Melbourne research team.
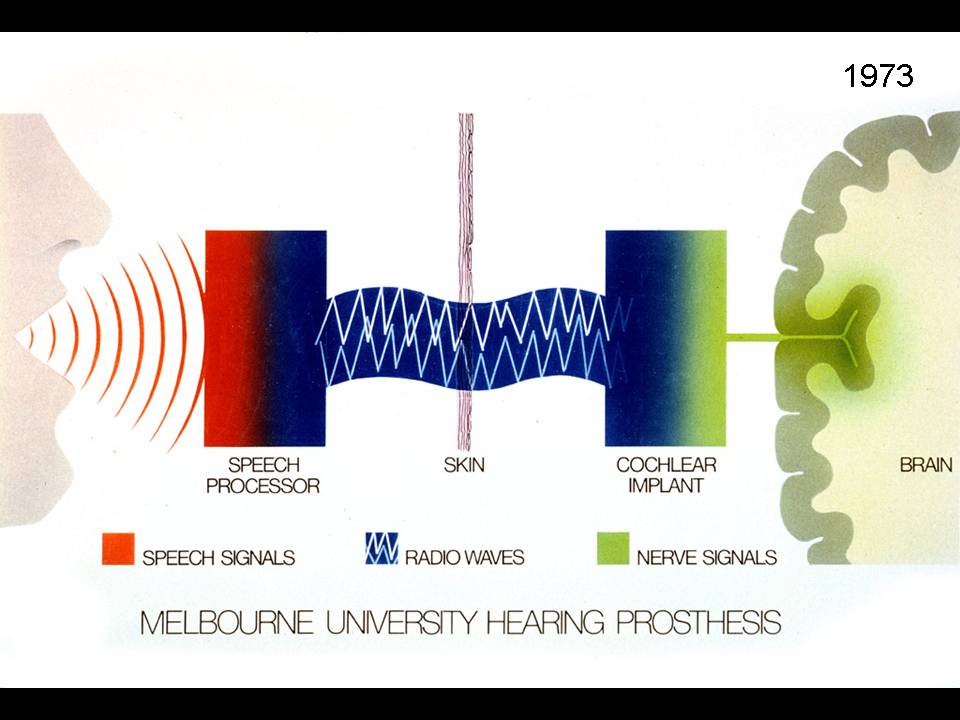 Notice sound is transmitted through the skin by radio-waves to a receiver implant, which decodes the signals and stimulates the different frequency regions of the brain on a place coding basis, and also transmits the lower frequencies for voicing.
Notice sound is transmitted through the skin by radio-waves to a receiver implant, which decodes the signals and stimulates the different frequency regions of the brain on a place coding basis, and also transmits the lower frequencies for voicing.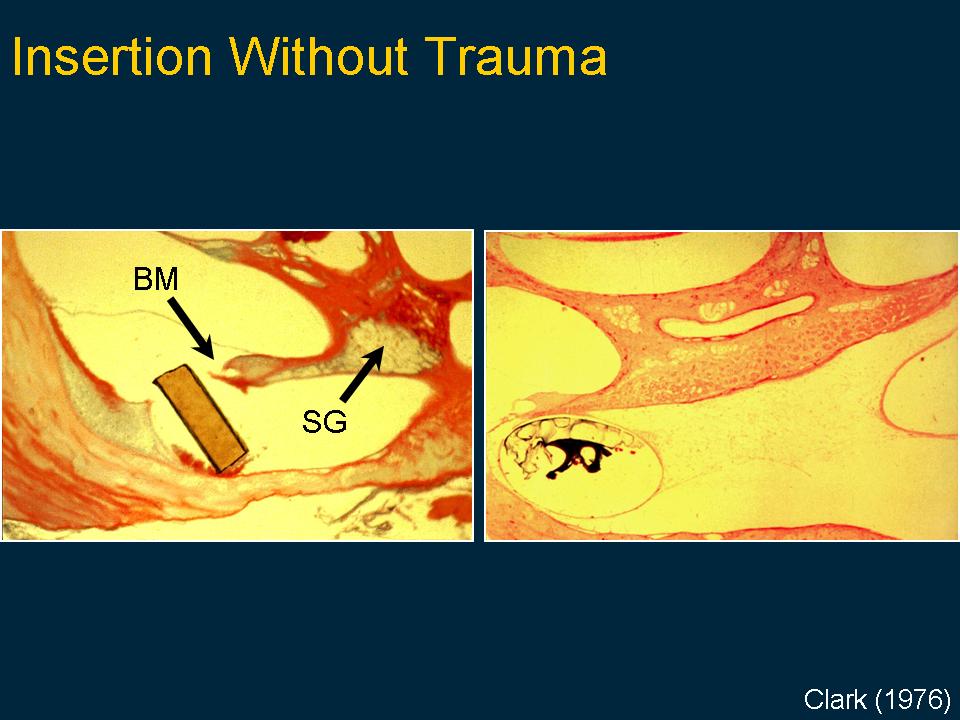 It meant also implanting electrodes inside the cochlea, which had to be checked carefully to see that it would be safe and that it would not lead to damaging the very inner ear structures it was important to stimulate. Here you can see how, if the electrode bundle cut through the fine vibrating membrane, the nerves would be damaged or destroyed. However it could be placed carefully and smoothly inside the inner ear and lie near the nerves.
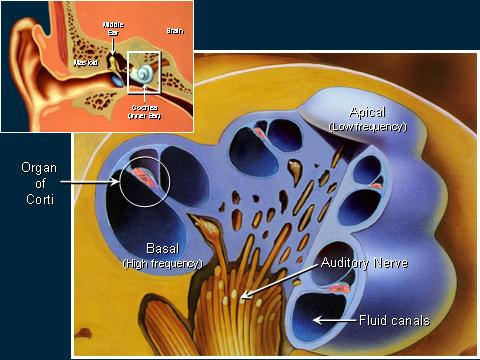
It meant also implanting electrodes inside the cochlea, which had to be checked carefully to see that it would be safe and that it would not lead to damaging the very inner ear structures it was important to stimulate. Here you can see how, if the electrode bundle cut through the fine vibrating membrane, the nerves would be damaged or destroyed. However it could be placed carefully and smoothly inside the inner ear and lie near the nerves.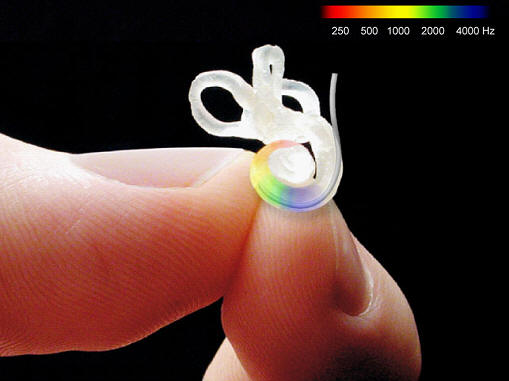 This image is a mould of the human cochlea showing how tiny it is. It has two and three quarter spirals around a central axis and the top loops for balance. The inner ear has three cavities which are about 1.5mm in diameter. There are up to 20,000 hair cells and 20,000 nerve fibres taking information to the brain. This was the challenge faced with a cochlear implant, how and what nerve to stimulate? The first evaluations on putting an electrode bundle into that spiral was that it would not pass up far enough to lie opposite the nerves transmitting speech frequencies. The answer came as shown in the next figure.
This image is a mould of the human cochlea showing how tiny it is. It has two and three quarter spirals around a central axis and the top loops for balance. The inner ear has three cavities which are about 1.5mm in diameter. There are up to 20,000 hair cells and 20,000 nerve fibres taking information to the brain. This was the challenge faced with a cochlear implant, how and what nerve to stimulate? The first evaluations on putting an electrode bundle into that spiral was that it would not pass up far enough to lie opposite the nerves transmitting speech frequencies. The answer came as shown in the next figure.
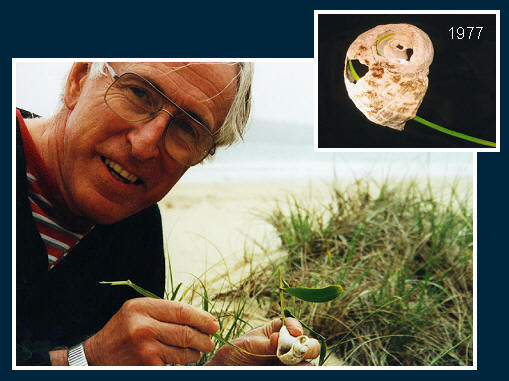 Clark made a discovery on the beach when examining a Turban Shell, and found that grass blades would go far enough around the spiral if they were flexible at the tip and stiffer at the base. This mechanical principle was applied to that used for electrodes for cochlear implants.
Clark made a discovery on the beach when examining a Turban Shell, and found that grass blades would go far enough around the spiral if they were flexible at the tip and stiffer at the base. This mechanical principle was applied to that used for electrodes for cochlear implants.
 His group also discovered that bands wrapped around the electrode made it smooth to pass easily up the cochlea and they were large enough to reduce the density of the electrical current to reduce damage to the nerve fibres.
His group also discovered that bands wrapped around the electrode made it smooth to pass easily up the cochlea and they were large enough to reduce the density of the electrical current to reduce damage to the nerve fibres.
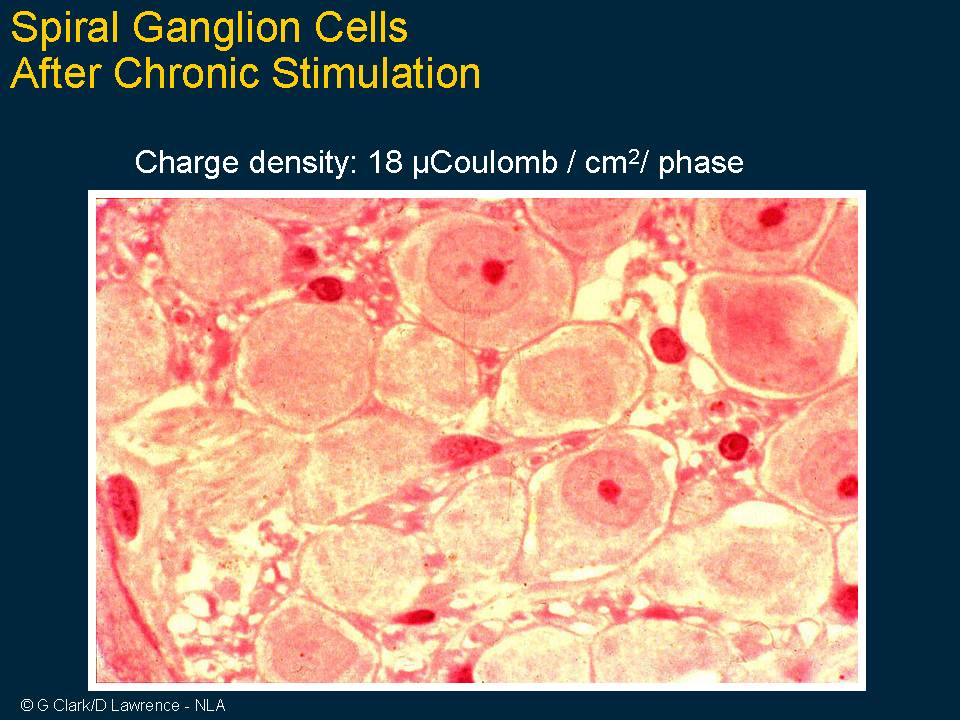 This slide shows the cell bodies of the auditory nerve in the inner ear after long periods of stimulation at intensity levels at the upper level of normal, and there is no damage, giving confidence that a cochlear implant would be safe.
This slide shows the cell bodies of the auditory nerve in the inner ear after long periods of stimulation at intensity levels at the upper level of normal, and there is no damage, giving confidence that a cochlear implant would be safe.
 It was also found by Clark and colleagues that middle ear infection could be limited in its spread to the inner ear if a tissue graft was taken and wrapped around the bundle where it went from the middle to the inner ear.
It was also found by Clark and colleagues that middle ear infection could be limited in its spread to the inner ear if a tissue graft was taken and wrapped around the bundle where it went from the middle to the inner ear.
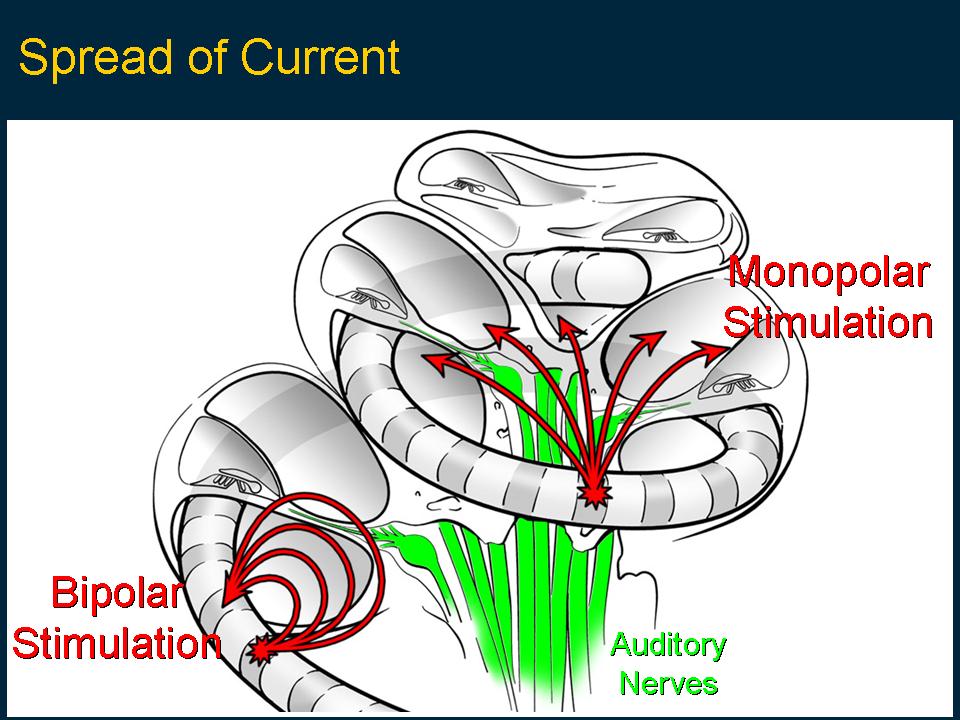 Another challenging research question was how to limit the spread of the current in the fluid-filled inner ear, so it would not short-circuit away from the nerves. This was needed in order to provide place coding for the high frequencies.
Another challenging research question was how to limit the spread of the current in the fluid-filled inner ear, so it would not short-circuit away from the nerves. This was needed in order to provide place coding for the high frequencies.
 The biological and physiological studies were important in designing a prototype cochlear implant for tests on initial patients. This slide demonstrates the circuitry needed for the first prototype receiver-stimulator which had 10 silicon chips marked with the circuit design as shown in the enlarged circuit layout.
The biological and physiological studies were important in designing a prototype cochlear implant for tests on initial patients. This slide demonstrates the circuitry needed for the first prototype receiver-stimulator which had 10 silicon chips marked with the circuit design as shown in the enlarged circuit layout.
 The receiver/stimulator needed to provide current pulses to the inner ear. It was first developed as a bench model shown here before it was integrated into a silicon chip and incorporated into the implanted package for the clinical trial.
The receiver/stimulator needed to provide current pulses to the inner ear. It was first developed as a bench model shown here before it was integrated into a silicon chip and incorporated into the implanted package for the clinical trial.
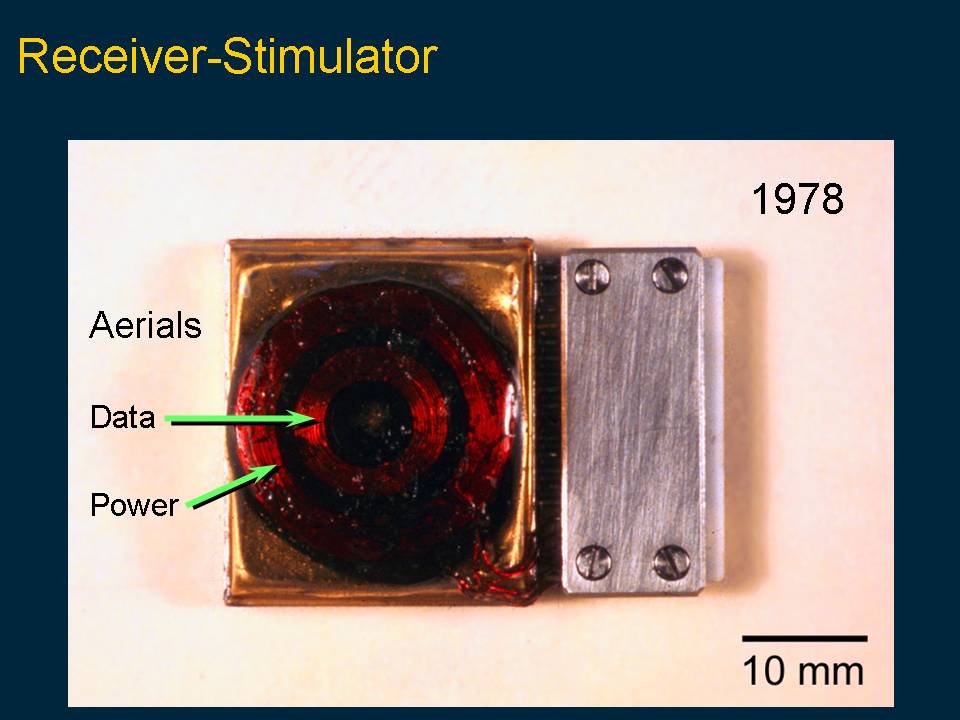 These slides show the first and second prototype receiver-stimulators used in the first patient on the 1st of August 1978 and 1979. They have two coils on the outside for receiving electro-conductive signals for power and also data.
These slides show the first and second prototype receiver-stimulators used in the first patient on the 1st of August 1978 and 1979. They have two coils on the outside for receiving electro-conductive signals for power and also data.

 The surgery was undertaken by the Head of the Unit, Professor Clark, and his surgical assistant Dr Brian Pyman at the Royal Victorian Eye and Ear Hospital in a flow of sterile air. Professor Clark is shown in the insert.
The surgery was undertaken by the Head of the Unit, Professor Clark, and his surgical assistant Dr Brian Pyman at the Royal Victorian Eye and Ear Hospital in a flow of sterile air. Professor Clark is shown in the insert.
 This is a photograph of the last stages of the first operation on Rod Saunders by Professor Clark and Dr Brian Pyman on the 1st of August 1978.
This is a photograph of the last stages of the first operation on Rod Saunders by Professor Clark and Dr Brian Pyman on the 1st of August 1978.
 This is a diagram of the electrode; free fitting bundle of 20 wires passed around the spiral of the cochlea to lie opposite the speech frequencies.
This is a diagram of the electrode; free fitting bundle of 20 wires passed around the spiral of the cochlea to lie opposite the speech frequencies.
 This is a photograph of the first patient Rod Saunders, three weeks after his surgery showing the incision.
This is a photograph of the first patient Rod Saunders, three weeks after his surgery showing the incision.
 This is an image of the computer used to develop a way of processing speech so it would get through a bottle neck to the brain and be heard as real speech signals. It was small by comparison to modern computers and had 16k of RAM.
This is an image of the computer used to develop a way of processing speech so it would get through a bottle neck to the brain and be heard as real speech signals. It was small by comparison to modern computers and had 16k of RAM.
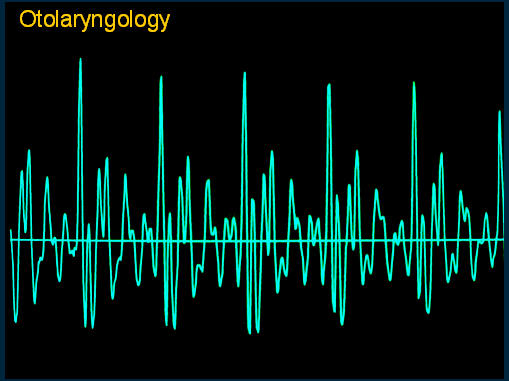 An illustration of a raw speech wave formed from part of the word ‘otolaryngology’ to illustrate how complex the signal is and the challenge facing the team to produce a code for transmitting to brain.
An illustration of a raw speech wave formed from part of the word ‘otolaryngology’ to illustrate how complex the signal is and the challenge facing the team to produce a code for transmitting to brain.
 The interesting finding in the first patient was that stimulating a certain location in the inner ear was heard as a sharp or dull sound. It gave timbre rather than pitch. Timbre is the description for a musical sound that plays the same note but on a different instrument, so it’s the quality of the sound.
The interesting finding in the first patient was that stimulating a certain location in the inner ear was heard as a sharp or dull sound. It gave timbre rather than pitch. Timbre is the description for a musical sound that plays the same note but on a different instrument, so it’s the quality of the sound.
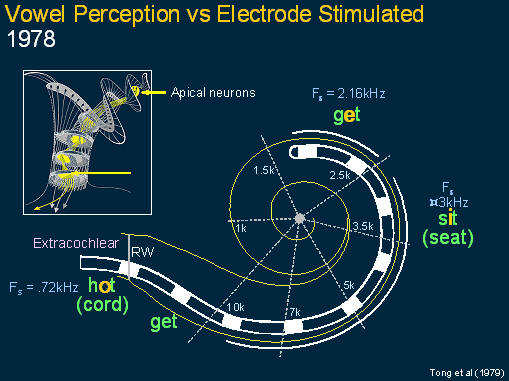 This slide shows a diagram of the cochlea and the first finding where the patient explained that stimulating different electrodes were heard not only as sharp and dull sounds but they were like vowels and the vowels varied according to the site of stimulation. It was noted that the frequency of site of stimulation corresponded to the frequency of a special signal in speech sounds called formants.
This slide shows a diagram of the cochlea and the first finding where the patient explained that stimulating different electrodes were heard not only as sharp and dull sounds but they were like vowels and the vowels varied according to the site of stimulation. It was noted that the frequency of site of stimulation corresponded to the frequency of a special signal in speech sounds called formants.
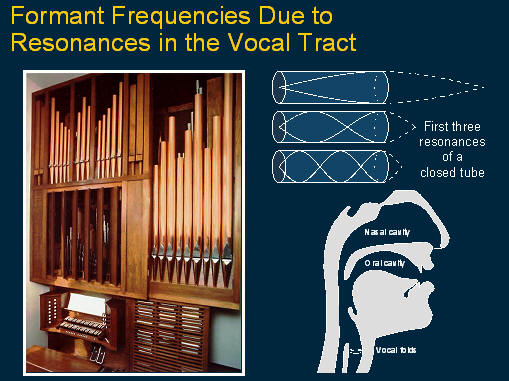 This shows an organ pipe arrangement to illustrate what a formant is. It’s a resonance in the vocal tract due to changes in dimensions with different speech sounds and conveys a lot of intelligibility. So the aim of the first processors was to select out the formants.
This shows an organ pipe arrangement to illustrate what a formant is. It’s a resonance in the vocal tract due to changes in dimensions with different speech sounds and conveys a lot of intelligibility. So the aim of the first processors was to select out the formants.
 This shows the first strategy: the second formant frequency which is very important for intelligibility was coded for place of stimulation and perceived by the brain as timbre. Sound pressure was coded as current level and perceived as loudness and the voicing frequency was coded and stimulus pulse rate and perceived as pitch, and it was transmitted across each site of electrical stimulation.
This shows the first strategy: the second formant frequency which is very important for intelligibility was coded for place of stimulation and perceived by the brain as timbre. Sound pressure was coded as current level and perceived as loudness and the voicing frequency was coded and stimulus pulse rate and perceived as pitch, and it was transmitted across each site of electrical stimulation.
 This illustrates that there are many features in speech signals that needed to be transmitted and coded. This speech spectrogram is for the word ‘bat’. Notice that the ‘b’ sound has a short burst of energy with different frequencies. The vowel ‘a’ has at least two strong bands of stimulation called the formants and the rate of stimulation relates to the voicing and the ‘t’ sound is a burst of high frequency energy.
This illustrates that there are many features in speech signals that needed to be transmitted and coded. This speech spectrogram is for the word ‘bat’. Notice that the ‘b’ sound has a short burst of energy with different frequencies. The vowel ‘a’ has at least two strong bands of stimulation called the formants and the rate of stimulation relates to the voicing and the ‘t’ sound is a burst of high frequency energy.
 Photograph showing Rod Saunders speaking with his wife using the first speech processor developed by the University of Melbourne’s Department of Otolaryngology.
Photograph showing Rod Saunders speaking with his wife using the first speech processor developed by the University of Melbourne’s Department of Otolaryngology.
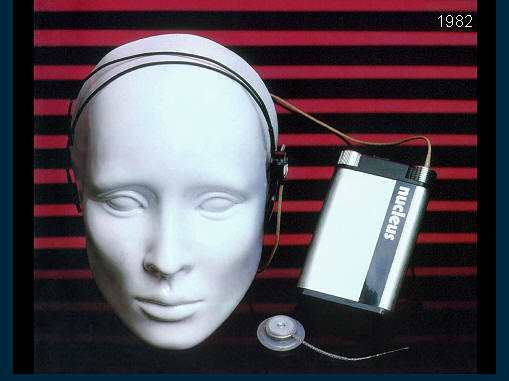 This slide shows the first commercially produced device by Nucleus later the company Cochlear Pty Ltd. It has a more reliable implant with a single coil and a smaller speech processor that’s still a headband to transmit signals through to the implant.
This slide shows the first commercially produced device by Nucleus later the company Cochlear Pty Ltd. It has a more reliable implant with a single coil and a smaller speech processor that’s still a headband to transmit signals through to the implant.
 When the world trial was carried out for the US Food and Drug Administration, it was shown to provide significant help when used in conjunction with lip reading and also provide help in understanding speech without lip-reading and electrical stimulation alone.
When the world trial was carried out for the US Food and Drug Administration, it was shown to provide significant help when used in conjunction with lip reading and also provide help in understanding speech without lip-reading and electrical stimulation alone.
 This graph shows the word correct scores for words and sentences with improvements in speech processing and it can be seen how for sentences the scores approximate 80% correct, which means the person can have a fluent conversation even without the need to lip read.
This graph shows the word correct scores for words and sentences with improvements in speech processing and it can be seen how for sentences the scores approximate 80% correct, which means the person can have a fluent conversation even without the need to lip read.
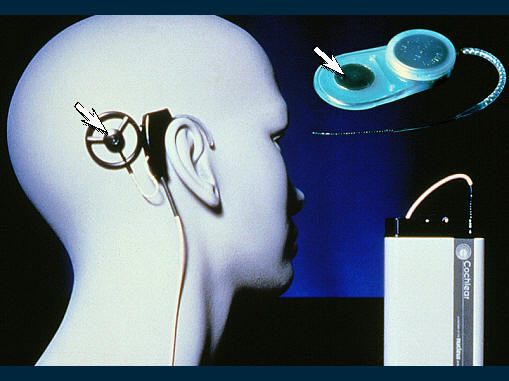 This image demonstrates the change in the system for operating on children in 1985. This implant has a magnet in the centre of the coils for receiving and transmitting information and that enabled children to apply it easily.
This image demonstrates the change in the system for operating on children in 1985. This implant has a magnet in the centre of the coils for receiving and transmitting information and that enabled children to apply it easily.
 When it was shown to be effective and safe for adults, Clark and colleagues undertook the first implants on children from 1985 through to 1986. This was after extra special safety precautions were evaluated to see that it was safe in this age group as they have special issues, and it was also made smaller and did not have a connector but a magnet on it to hold the transmitting coil in place. This is an image of the first two young children operated on in 1985 and 1986.
When it was shown to be effective and safe for adults, Clark and colleagues undertook the first implants on children from 1985 through to 1986. This was after extra special safety precautions were evaluated to see that it was safe in this age group as they have special issues, and it was also made smaller and did not have a connector but a magnet on it to hold the transmitting coil in place. This is an image of the first two young children operated on in 1985 and 1986.
 Then in 1987 a world trial was commenced for the US FDA on children from two to 17 years of age. These are the best perceptual categories achieved for closed and open-set words both before and after electrical stimulation. Note the high proportion obtaining open or closed set speech understanding for electrical stimulation alone.
Then in 1987 a world trial was commenced for the US FDA on children from two to 17 years of age. These are the best perceptual categories achieved for closed and open-set words both before and after electrical stimulation. Note the high proportion obtaining open or closed set speech understanding for electrical stimulation alone.
In 1990 the FDA announced that the 22-channel cochlear implant was safe and effective for deaf children from two to 17 years of age in understanding speech both with and without lipreading. It was the first cochlear implant to be approved for deaf children by any world regulatory body.
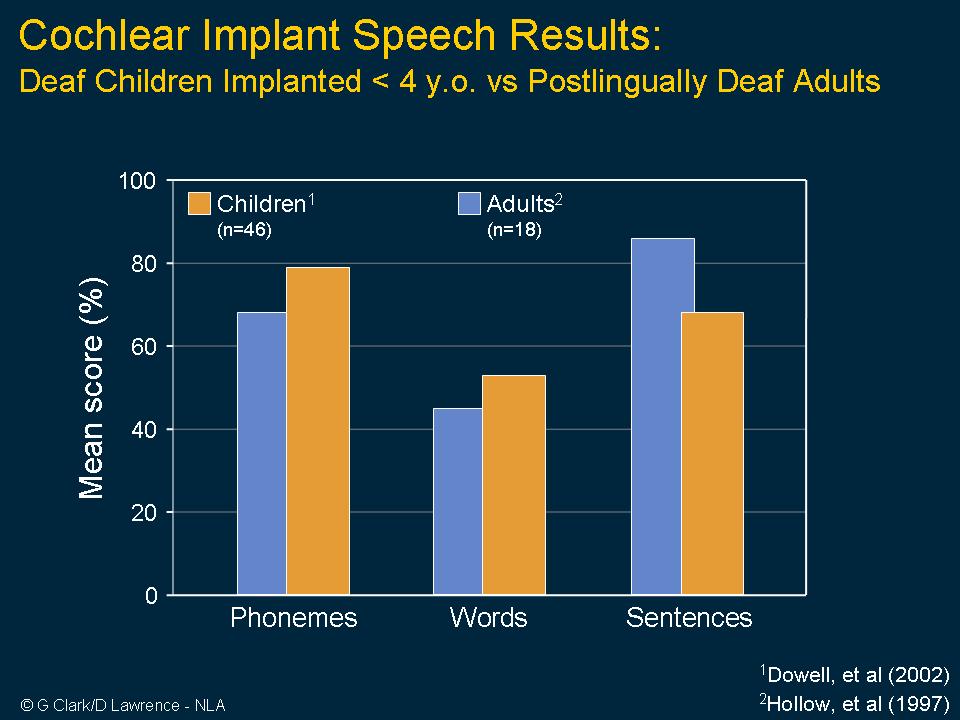 The results in children were shown to be similar to those of adults who had had hearing before going deaf. The special safety issues were head growth and also the risk of middle ear infection leading to meningitis.
The results in children were shown to be similar to those of adults who had had hearing before going deaf. The special safety issues were head growth and also the risk of middle ear infection leading to meningitis.
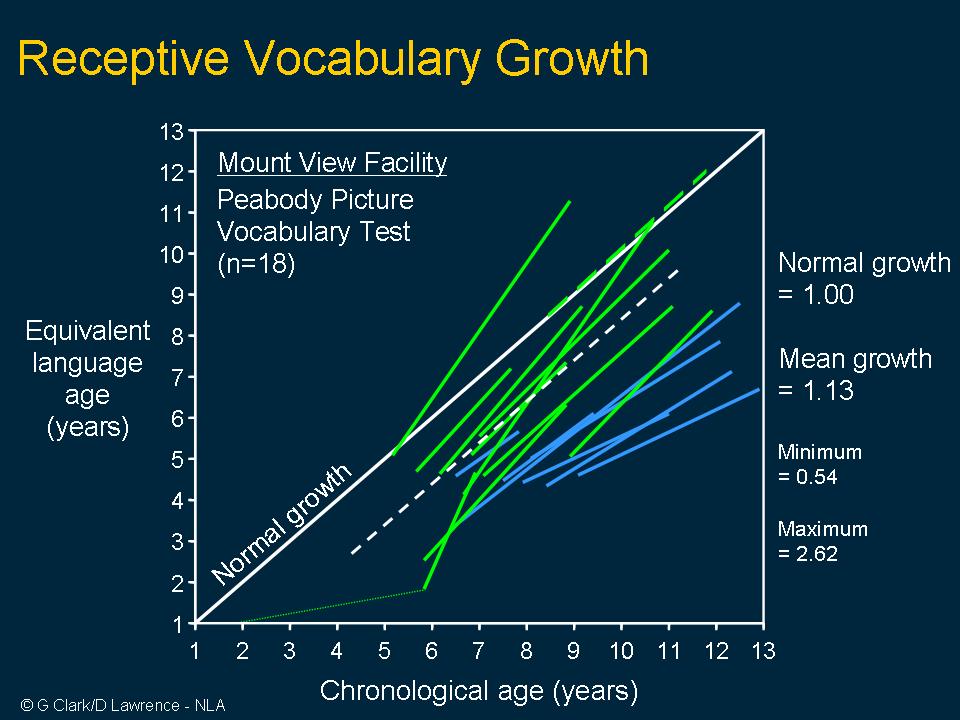 In the children who were evaluated by centres in Melbourne and around the world, the children not only developed the ability to understand speech but also their spoken language in many cases reached normal levels for children with hearing.
In the children who were evaluated by centres in Melbourne and around the world, the children not only developed the ability to understand speech but also their spoken language in many cases reached normal levels for children with hearing.
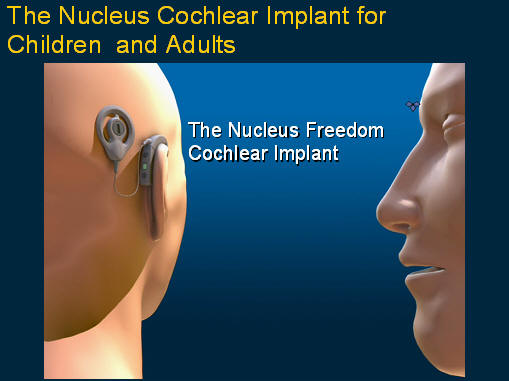 This image shows a demonstration of how the latest the Nucleus Freedom cochlear implant works.
This image shows a demonstration of how the latest the Nucleus Freedom cochlear implant works.